Pop Culture Coding Case Studies: The Pitt (Season 1 – Episode 1)
Welcome to the Pop Culture Coding Challenge!
If you are a fan of the medical drama The Pitt, you know the Emergency Department is always chaotic, the patients are critically ill, and the doctors are moving fast. But what happens after the episode ends and the chart goes to the billing department? That is where coders come in!
In today's scenario, we have a Good Samaritan who jumped onto the "T" railway tracks to save an assault victim, only to suffer a severe injury himself. This case is packed with trauma coding rules, critical care time calculations, and a sneaky "Documentation Trap."
Disclaimer: The following is a completely fictional medical record created for educational purposes based on characters and events from a television show. No actual patient information (PHI) is included.
The Clinical Scenario
EMERGENCY DEPARTMENT EXAM AND TREATMENT NOTE
Patient Name: Samuel "Sam" Wallace
Age/Sex: Adult Male
Chief Complaint: Head trauma, unresponsiveness.
History of Present Illness (HPI): Patient is brought in by EMS as a Level 1 Trauma. Per bystander reports, the patient jumped down onto the "T" railway tracks to rescue an elderly woman who had been pushed. After assisting her, he attempted to climb back up to the platform, slipped, and fell backward, striking his head on the tracks. He was unresponsive at the scene. EMS noted agonal respirations and initiated bag-valve-mask ventilation en route. Past Medical History: No records in PTMC system. Dr. Mohan assumes patient is likely on anticoagulants due to age and presentation, but this cannot be confirmed at this time.
Physical Examination (07:00 A.M.):
- Vitals: HR 55 | BP 160/90 | RR 6 (Agonal) | SpO2 88% on BVM
- General: Unresponsive, comatose.
- Neurological: GCS 3. Pupils are sluggish but equal.
- Head/ENT: Large hematoma and abrasion to the left occipitotemporal region.
Procedures: Endotracheal Intubation (07:05 A.M.): Due to agonal respirations, hypoxia, and inability to protect his airway (GCS 3), the decision was made to intubate. Pre-oxygenated with 100% O2. Using a Mac 3 blade and direct laryngoscopy, the vocal cords were visualized, and a size 8.0 endotracheal tube was passed through the cords without difficulty. Placement confirmed by bilateral breath sounds, equal chest rise, and positive end-tidal CO2 color change. Tube secured at 22 cm at the lip.
Emergency Department Course & Medical Decision Making (MDM): Patient stabilized post-intubation and placed on mechanical ventilation. Stat trauma labs and CT scans ordered.
- Imaging Results: Head CT (Non-contrast) shows a small left temporal intraparenchymal bleed. No epidural hematoma. No subdural hematoma. No midline shift.
09:00 A.M. - Patient remains comatose but hemodynamically stable. 10:00 A.M. - Vitals stable. Hourly neuro checks ongoing. 11:00 A.M. - Repeat Head CT performed. Results show the intraparenchymal hemorrhage is stable with no extension. 12:30 P.M. - Sedation holiday initiated. Patient began waking up, opening eyes spontaneously, and following commands. Patient was successfully extubated. 13:00 P.M. - Patient is awake, alert, and conversing appropriately with staff and law enforcement.
Final Assessment & Diagnoses:
- Traumatic Left Temporal Intraparenchymal Hemorrhage: Confirmed on CT. Patient suffered a severe closed head injury after a fall from a height onto the railway tracks. Patient experienced a prolonged Loss of Consciousness (LOC) lasting approximately 5.5 hours from the time of injury until extubation.
- Acute Respiratory Failure: Patient arrived comatose with agonal respirations and hypoxia secondary to the traumatic brain injury, requiring emergent endotracheal intubation and mechanical ventilation. Patient was successfully weaned and extubated in the ED.
- Coma (GCS 3 on arrival): Resolved. Patient is currently awake, alert, and oriented x4.
- Mechanism of Injury: Accidental fall from a platform onto train tracks after jumping down to assist an assault victim.
CRITICAL CARE ATTESTATION: I spent a total of 85 minutes of critical care time exclusively directing the care of this critically ill trauma patient. This time included bedside evaluation, ventilator management, coordinating ICU admission, reviewing serial CT scans, and performing serial neurological exams to monitor for brain herniation. This time does NOT include the time spent performing the endotracheal intubation.
Your Coding Challenge:
Grab your codebooks! Based on the ED note above, try to determine:
- The correct Evaluation & Management (E/M) code(s) for the physician. (Hint: Look closely at the total time in the attestation!)
- The CPT procedure code for the airway management.
- The ICD-10-CM diagnosis codes, including the External Cause codes for how and where he got hurt!
Click Here To Reveal Answers & Rationale!
- Physician E/M & Procedures (Professional Billing)
- CPT 99291-25 – Critical care, first 30-74 minutes.
- CPT 99292 – Critical care, each additional 30 minutes.
- Teaching Rationale: The physician documented 85 minutes of critical care time. The first 74 minutes maxes out code 99291. Once you hit minute 75, you get to add 99292 for the additional time! Modifier 25 goes on the primary E/M code to show it's separate from the intubation.
- CPT 31500 – Intubation, endotracheal, emergency procedure.
- Teaching Trap: Did you try to code the extubation (removing the tube) at 12:30 P.M.? Extubation is considered an inclusive component of overall airway management and is not billed separately!
- Teaching Trap: Did you try to code the extubation (removing the tube) at 12:30 P.M.? Extubation is considered an inclusive component of overall airway management and is not billed separately!
- ICD-10-CM Diagnosis Codes
- Primary: S06.393A – Other focal traumatic brain injury with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter. (Because Dr. Mohan documented exactly 5.5 hours of LOC, we can code to this specific 6th character)
- J96.01 – Acute respiratory failure with hypoxia.
- R40.2430 – Glasgow coma scale score 3, at arrival.
- External Cause: W17.89XA – Other fall from one level to another, initial encounter.
- Place of Occurrence: Y92.522 – Railway station as the place of occurrence of the external cause.
💡 Pro-Coder Tip: Specificity is King! You might initially find Y92.89 (Other specified places) if you just look up "Railway track" in the index. However, the note mentions Sam jumped from a "platform" while waiting for the "T" transit train. Because this happened at a station, Y92.522 is the most accurate choice!
⚠️ The "Documentation Trap" (Did you catch it?): Did you try to code Z79.01 (Long term current use of anticoagulants)? Dr. Mohan stated she assumes he is anticoagulated, but they have no records to prove it. If it isn't confirmed, it isn't coded!
🧠 Anatomy Break: Where is a "Left Temporal Intraparenchymal" Bleed?
In the ER, Dr. Mohan notes that Sam has a "small left temporal intraparenchymal bleed," but specifically mentions there is "no epidural and no subdural" hematoma. As a medical coder, you cannot just code a generic "head bleed"—you need to know exactly what these anatomical terms mean to get to the right ICD-10-CM category!
Let's break the medical term down into two parts: the lobe and the layer.
- "Left Temporal" (The Lobe) The brain is divided into distinct sections called lobes. The Temporal Lobe is located on the side of the brain, sitting roughly behind your temples and just above your ears. Because Sam hit the left side of his head when he fell backward onto the tracks, the injury is localized to the left temporal lobe. (Fun clinical fact: The left temporal lobe is heavily involved in language, hearing, and memory!)
- "Intraparenchymal" (The Layer) This is the most important part for a trauma coder to understand! The skull has several protective layers (meninges) between the bone and the brain. Where the blood pools determines your exact diagnosis code:
- "Intra" means inside or within.
- "Parenchyma" refers to the actual, functional tissue of an organ (in this case, the brain tissue itself).
- Therefore, an Intraparenchymal bleed means the blood vessel ruptured deep inside the actual brain tissue.
The Coding Connection: This anatomy lesson directly dictates your code path!
- If the bleed was outside the brain tissue but trapped under the skull (like an Epidural or Subdural hematoma), you would be directed to the S06.4- or S06.5- code categories.
- Because Sam's bleed is inside the brain tissue itself (Intraparenchymal), the ICD-10-CM index classifies it as a "Focal Traumatic Brain Injury," which directs you specifically to the S06.3- category that we used in our Answer Key!
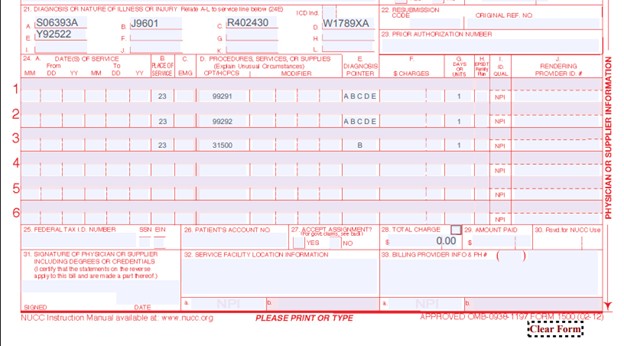
Taking It to the Claim Form: The CMS-1500
How does this look in the real world? Here is exactly how we map Sam's codes onto the physician's CMS-1500 claim form to prove medical necessity.
Box 21 (Diagnosis Codes):
- S06393A
- J9601
- R402430
- W1789XA
- Y92522
Box 24 (Procedures & Diagnosis Pointers):
- Line 1: 99291-25 points to A B C D E (The critical care treats the whole patient and the trauma).
- Line 2: 99292 points to A B C D E (The extra critical care time).
- Line 3: 31500 points to B > 💡 Why does Line 3 only point to "B"?
As a coder, you must explicitly link the procedure to the specific diagnosis that makes it medically necessary. The physician placed the breathing tube specifically to treat the Acute Respiratory Failure (B)!
Real-World Reality Check: Paper vs. Electronic Claims
We use the classic, red-ink CMS-1500 form in our exercises because it is the absolute best visual tool to learn where coding data belongs and how procedures link to diagnoses.
However, when you land your first job as a medical coder, you won't be using a typewriter! In the real world, you will enter these CPT and ICD-10 codes directly into a hospital's Electronic Health Record (EHR) or Practice Management software such as Epic.
Once you click "Submit," the software automatically takes the data from your screen, maps it to the exact same "boxes" you see on this paper form, and converts it into a secure digital file called an EDI 837P (Electronic Data Interchange) to send to the insurance company instantly.