Pop Culture Coding Case Studies: The Pitt (Season 1 – Episode 6)
Welcome to the Pop Culture Coding Challenge!
If you are a fan of the medical drama The Pitt, you know the Emergency Department is a pressure cooker where every second counts. But once the patient is stabilized and the sirens fade, the real work begins for the Revenue Cycle Team.
In today’s scenario, we are stepping into the shoes of Dr. Heather Collins as she manages a high-stakes surgical emergency: Testicular Torsion. When 16-year-old Dillon Chambers arrives in agonizing pain, the clock is ticking to save an organ. This case is a masterclass in:
- High-Acuity MDM: How to leverage an "acute threat to organ life" to justify a high E&M level.
- The APC Bundle Trap: Why choosing to "roll" a procedure into the E/M is often a smarter financial move than billing it separately.
- Revenue Integrity: Correctly billing for multiple bedside ultrasounds (POCUS) using specific modifiers to capture the doctor's expert interpretation.
Disclaimer: The following is a completely fictional medical record created for educational purposes based on characters and events from a television show. No actual patient information (PHI) is included.
The Clinical Scenario
EMERGENCY DEPARTMENT EXAM AND TREATMENT NOTE
PATIENT: Chambers, Dillon | DOB: 05/12/2010 | AGE: 16
DATE OF SERVICE: 09/05/2025 | TIME: 12:00 P.M.
I. CLINICAL PRESENTATION
CHIEF COMPLAINT: Sudden onset of severe (10/10) scrotal pain.
HISTORY of PRESENT ILLNESS: 16-year-old male presents with acute, non-traumatic scrotal pain starting 60 minutes prior to arrival. Patient reports associated nausea and one episode of emesis. He is visibly distressed.
PHYSICAL EXAM: Left scrotum is edematous and erythematous. Left testis is in a high-lie, transverse position. Absent cremasteric reflex on the left.
II. DIAGNOSTIC INTERPRETATION
SCROTAL ULTRASOUND (POCUS): Results show a complete absence of blood flow to the left testicle with a "whirlpool sign" noted at the spermatic cord. Findings diagnostic for acute torsion.
III. PROCEDURE: MANUAL DETORSION
PRE-PROCEDURE SEDATION: Intranasal Midazolam administered for pain/anxiety.
INFORMED CONSENT: Patient and mother were counseled on the risks of manual detorsion (failure to reduce, persistent ischemia) and the necessity of subsequent surgery. Risks of upcoming urology surgery including infection, hematoma, and potential orchiectomy (testicular loss) were explained. All questions were answered; consent was obtained.
TECHNIQUE: The left testicle was manually rotated 180° in a medial-to-lateral ("open book") direction.
OUTCOME: Patient reported immediate significant relief (pain decreased 10/10 to 3/10). Repeat bedside Doppler confirmed a return of robust arterial flow.
IV. COORDINATION OF CARE & PLAN
CONSULTATION: Case discussed via telephone with Dr. Vance (Urology). Doppler findings and successful manual reduction were reviewed.
PLAN: Patient is admitted to the Urology service. He remains NPO and is scheduled for an urgent bilateral orchiopexy (surgical fixation) at 2:00 P.M. to prevent recurrence.
DIAGNOSIS: Left Torsion of the Spermatic Cord (Reduced).
Electronically Signed by Heather Collins, MD
Think Like a Coder, Bill Like an Expert. >
Use the clinical facts in the scenario to build a claim that survives the "Claim Scrubber" and defends the hospital’s bottom line.
- Diagnosis Selection: What is the First-Listed (Primary) Diagnosis for this encounter?
- E/M Leveling: Based on the 2023 MDM guidelines, what level of Emergency Department E/M is supported?
- The Procedure Puzzle: There is no dedicated CPT code for manual detorsion. Which surgical CPT and modifier combination would you use to represent this work?
- Ancillary Services: Which CPT code and specific modifiers are required to report the bedside ultrasounds performed by Dr. Collins?
Click Here To Reveal Answers & Rationale!
SMK CODING CHALLENGE: THE ANSWER KEY
-
ICD-10-CM: The Diagnosis
Primary Code: N44.02
Description: Intravaginal torsion of spermatic cord.
The Alphabetic Index Path: Torsion – spermatic cord.
Rationale: The ICD-10-CM tabular list includes an Inclusion Note under N44.02 for "Torsion of spermatic cord NOS." Because the provider documented "Torsion of the spermatic cord" and the patient is an adolescent, this is the default, clinically appropriate code.
Did You Know?" In Latin, vagina means "sheath." Intravaginal torsion means the cord twisted inside the protective sheath (Tunica Vaginalis) covering the testicle. -
CPT: Professional Services (Physician Billing)
- CPT Code: 99285
Modifier(s): N/A
Description: Emergency Department Visit, Level 5. No Modifier 25 is needed because diagnostic radiology does not bundle with E&M services. - CPT Code: 76870
Modifier(s): -26
Description: Ultrasound, scrotum and contents. Modifier -26 represents the Professional Component (Dr. Collins’ interpretation and report). - CPT Code: 76870
Modifier(s): -26, -76
Description: Repeat Ultrasound, scrotum and contents. Modifier -76 indicates a repeat procedure by the same physician to confirm blood flow returned after the detorsion.
- CPT Code: 99285
-
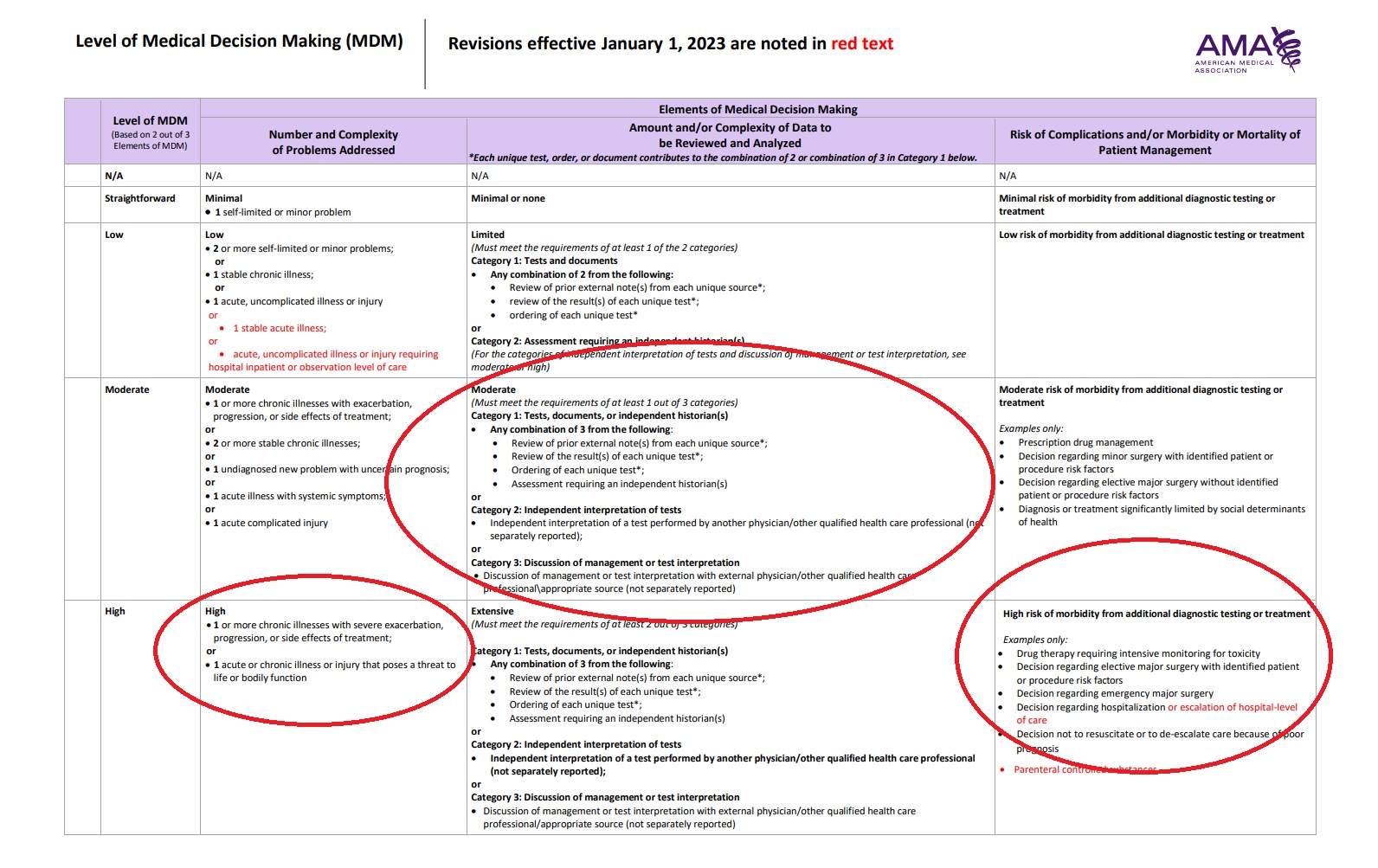
MDM Table Logic: The "2 out of 3" Rule
Problem Complexity (HIGH): Acute illness posing a threat to bodily function (organ loss).
Data Complexity (MODERATE): * Category 1: Ordering of unique tests (x2). (Note: We do not count the review because we are billing the -26 professional fees separately).
Category 3: Discussion of management with an external specialist (Urologist).
Risk of Management (HIGH): Includes the decision for emergency major surgery and the high-risk manual detorsion. -
The Policy Choice: To Bill or to Bundle?
"Wait, couldn't I bill a CPT code for the manual untwisting?"
Since CPT does not provide a dedicated code for non-surgical manipulation, you can report 54600-52 to capture the essential work of the "Reduction of torsion" while using the Reduced Services modifier to indicate the procedure was performed manually rather than through a traditional surgical incision.
In a hospital setting, CPT 54600 (Reduction of torsion) is bundled into the APC rate (Ambulatory Payment Classification) for the definitive surgical repair performed later that day by the Urologist.
Billing 54600 would result in $0 additional reimbursement. Instead, we "roll" that work into our E/M to support the High-Risk requirements of a 99285, ensuring the hospital is paid fairly for Dr. Collins' expertise and high-stakes intervention. -
Compliance Corner: The Modifier 76 Rule
Without Modifier 76 on that second ultrasound, the insurance company's "Claim Scrubber" would automatically delete the second charge as a duplicate. The -76 tells the payer: "I did this twice because I needed to make sure the blood was flowing again!"
Mapping the 99285" > Use the table below to see exactly how we applied the '2 out of 3' rule. Notice which columns hit 'High' and which stayed at 'Moderate' and why the final code is a 99285.